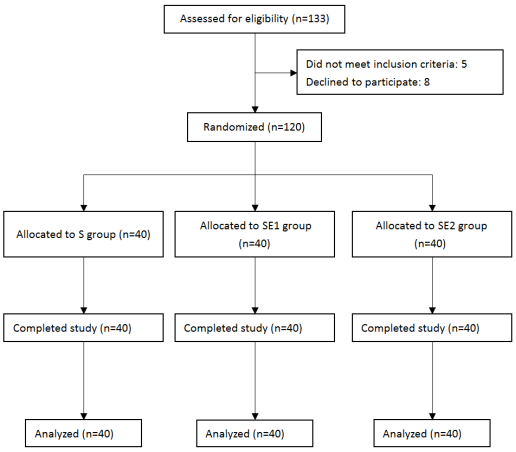
Background: Total hip arthroplasty (THA) is a common procedure for end-stage hip disorders, yet postoperative pain management remains challenging due to opioid-related complications, particularly in elderly patients vulnerable to respiratory depression and delirium. Multimodal analgesia strategies are increasingly prioritized to mitigate these risks. Esketamine, an NMDA receptor antagonist with opioid-sparing and anti-neuroinflammatory properties, shows promise in enhancing analgesia while reducing adverse effects. Preliminary studies suggest its efficacy in lowering postoperative pain and delirium risk, though optimal dosing in elderly THA populations remains unclear. This study aimed to evaluate the analgesic efficacy and safety of different dosages of esketamine combined with sufen-tanil for patient-controlled intravenous analgesia (PCIA) in elderly patients undergoing total hip arthroplasty. Methods: In this randomized, prospective, double-blind trial, 120 elderly patients were randomly divided into three groups: the control group (Group S, n = 40) received sufentanil 2 μg/kg; the experimental group SE1 (n = 40) received sufentanil 1.5 μg/kg combined with esketamine 1 mg/kg; and the experimental group SE2 (n = 40) received sufentanil 1 μg/kg combined with esketamine 2 mg/kg. Primary outcomes included resting and movement-associated Visual Analogue Scale (VAS) scores at 4, 8, 12, 24, and 48 h postoperatively. Secondary outcomes encompassed Ramsay Sedation Scale (RSS) scores, Quality of Recovery-15 (QoR-15) scores at 48 h, time to first walk, the number of patients requiring remedial analgesia, and adverse events (nausea/vomiting, hallucinations, pruritus, delirium, dizziness). Results: The SE1 and SE2 groups demonstrated significantly superior analgesic efficacy compared to the S group across all outcomes. Resting and movement-associated VAS scores were significantly lower in both esketamine-combined groups at all postoperative time points (4, 8, 12, 24, and 48 h; P < 0.05). Sedation levels (Ramsay scores) were dose-dependently enhanced with esketamine. Group SE2 exhibited higher sedation scores than Group S at 24 h (P < 0.01) and 48 h (P < 0.05). The QoR-15 scores at 48 h were significantly higher in Groups SE1 and SE2 compared to Group S (P < 0.001). Time to first walk was shorter in Groups SE1 and SE2 than in Group S (P < 0.001). No significant differences were observed in the requirement for rescue analgesia between groups. Adverse events showed a significant reduction in postoperative delirium (POD) incidence (P < 0.01) and nausea/vomiting (P < 0.05) in Groups SE1 and SE2 compared to Group S, with no significant differences in dizziness, hallucinations, or pruritus. Conclusion: This randomized controlled trial demonstrated that esketamine combined with reduced-dose sufentanil significantly improved postoperative analgesia and recovery outcomes in elderly patients undergoing THA.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 13, Issue 1) |
| DOI | 10.11648/j.ijacm.20251301.16 |
| Page(s) | 37-45 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Esketamine, Sufentanil, Total Hip Arthroplasty, Patient-Controlled Intravenous Analgesia, Postoperative Pain
Variable | S Group (n=40) | SE1 Group (n=40) | SE2 Group (n=40) | p-value |
|---|---|---|---|---|
Age (years) | 73.8 ± 7.6 | 75.5 ± 8.3 | 72.2 ± 7.9 | 0.181 |
Female (n, %) | 22 (55.0%) | 25 (62.5%) | 20 (50.0%) | 0.526 |
Height (cm) | 157.9 ± 6.8 | 159.1 ± 7.1 | 156.8 ± 6.5 | 0.322 |
Weight (kg) | 55.2 ± 7.5 | 56.8 ± 8.2 | 54.5 ± 6.9 | 0.380 |
ASA classification (n, %) | 0.705 | |||
ASA 1 | 8 (20.0%) | 5 (12.5%) | 6 (15.0%) | |
ASA 2 | 26 (65.0%) | 28 (70.0%) | 24 (60.0%) | |
ASA 3 | 6 (15.0%) | 7 (17.5%) | 10 (25.0%) | |
Hypertension (n, %) | 24 (60.0%) | 28 (70.0%) | 25 (62.5%) | 0.623 |
Diabetes (n, %) | 17 (42.5%) | 13 (32.5%) | 15 (37.5%) | 0.652 |
Operation time (min) | 94.5 ± 13.8 | 89.2 ± 12.9 | 91.7 ± 14.1 | 0.212 |
Intraoperative blood loss (ml) | 305 ± 56 | 320 ± 47 | 300 ± 52 | 0.203 |
Assessment | Time | S Group | SE1 Group | SE2 Group | P (ANOVA) | Pairwise Comparisons (P; Cohen’s d) | η² |
|---|---|---|---|---|---|---|---|
Resting VAS | 4h | 4.97 ± 0.78 | 4.65 ± 0.89 | 4.42 ± 0.57 | 0.006 | S-SE2: 0.005 (0.77) | 0.083 |
8h | 5.01 ± 0.72 | 4.77 ± 0.70 | 4.51 ± 0.64 | 0.007 | S-SE2: 0.011 (0.74) | 0.081 | |
12h | 4.71 ± 0.63 | 4.49 ± 0.73 | 4.30 ± 0.68 | 0.030 | S-SE2: 0.022 (0.60) | 0.058 | |
24h | 4.01 ± 0.53 | 3.81 ± 0.47 | 3.68 ± 0.49 | 0.013 | S-SE2: 0.012 (0.67) | 0.071 | |
48h | 3.01 ± 0.36 | 2.86 ± 0.29 | 2.79 ± 0.32 | 0.010 | S-SE1: 0.039 (0.46); S-SE2: 0.003 (0.69) | 0.076 | |
Movement VAS | 4h | 5.86 ± 0.79 | 5.62 ± 0.71 | 5.39 ± 0.83 | 0.029 | S-SE2: 0.002 (0.58) | 0.059 |
8h | 5.92 ± 0.81 | 5.66 ± 0.75 | 5.48 ± 0.79 | 0.022 | S-SE2: 0.019 (0.57) | 0.063 | |
12h | 6.23 ± 0.97 | 5.84 ± 0.83 | 5.71 ± 0.91 | 0.035 | S-SE2: 0.035 (0.55) | 0.055 | |
24h | 5.18 ± 0.85 | 4.93 ± 0.66 | 4.72 ± 0.69 | 0.023 | S-SE2: 0.001 (0.60) | 0.063 | |
48h | 5.01 ± 0.82 | 4.65 ± 0.78 | 4.41 ± 0.62 | 0.002 | S-SE1: 0.012 (0.45); S-SE2: <0.001 (0.78) | 0.101 |
Outcome | Time | S Group | SE1 Group | SE2 Group | P-value | Effect Size (η²) |
|---|---|---|---|---|---|---|
Ramsay Sedation Score | 4h | 2.75 ± 0.41 | 2.87 ± 0.39 | 2.91 ± 0.45 | 0.206 | NS |
8h | 2.79 ± 0.45 | 2.93 ± 0.58 | 3.02 ± 0.61 | 0.175 | NS | |
12h | 2.98 ± 0.52 | 3.15 ± 0.49 | 3.21 ± 0.43 | 0.090 | NS | |
24h | 2.85 ± 0.56 | 3.09 ± 0.58 | 3.19 ± 0.50 | 0.009 | 0.078 | |
48h | 2.81 ± 0.47 | 2.99 ± 0.48 | 3.14 ± 0.62 | 0.022 | 0.063 | |
QoR-15 | 48h | 114.7 ± 3.92 | 118.8 ± 4.79 | 120.2 ± 4.51 | <0.001 | 0.700 |
Time to First Ambulation (h) | - | 49.65 ± 4.72 | 46.36 ± 3.89 | 45.53 ± 4.02 | <0.001 | 0.154 |
Rescue Analgesia (n) | - | 2 (5.0%) | 1 (2.5%) | 0 (0.0%) | 0.368 | NS |
Adverse Event | S Group (n=40) | SE1 Group (n=40) | SE2 Group (n=40) | P-value | Significant Pairwise Comparisons (P-value; Cohen’s V) |
|---|---|---|---|---|---|
Nausea/Vomiting | 16 (40.0%) | 7 (17.5%) | 6 (15.0%) | 0.016 | S-SE1: 0.039 (V=0.26); S-SE2: 0.024 (V=0.28) |
Hallucination | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | N/A | Not applicable |
Pruritus | 3 (7.5%) | 2 (5.0%) | 2 (5.0%) | 0.895 | NS |
Delirium | 17 (42.5%) | 6 (15.0%) | 7 (17.5%) | 0.007 | S-SE1: 0.013 (V=0.28); S-SE2: 0.025 (V=0.25) |
Dizziness | 13 (32.5%) | 8 (20.0%) | 6 (15.0%) | 0.109 | NS |
THA | Total Hip Arthroplasty |
PCIA | Patient-controlled Intravenous Analgesia |
VAS | Visual Analogue Scale |
RSS | Ramsay Sedation Scale |
QoR-15 | Quality of Recovery-15 |
POD | Postoperative Delirium |
PONV | Postoperative Nausea and Vomiting |
NMDA | N-methyl-D-aspartate |
POND | Postoperative Neurocognitive Disorders |
ASA | American Society of Anesthesiologists |
NYHA | New York Heart Association |
LVEF | Left Ventricular Ejection Fractions |
LMA | Laryngeal Mask Airway |
IBP | Invasive Arterial Blood Pressure |
BIS | Bispectral Index |
| [1] | Kurtz S, Ong K, Lau E, Mowat F, Halpern M: Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 2007, 89(4): 780-785. |
| [2] | Højer Karlsen AP, Geisler A, Petersen PL, Mathiesen O, Dahl JB: Postoperative pain treatment after total hip arthroplasty: a systematic review. Pain 2015, 156(1): 8-30. |
| [3] | Yang N, Wuhuzi W, Guo X, Li Y, Zhang X: [Analgesic effect of "cocktail" analgesia containing high-dose compound betamethasone after revision hip arthroplasty and the use of opioid drugs]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2025, 39(3): 314-319. |
| [4] | Mangoni AA, Jackson SH: Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol 2004, 57(1): 6-14. |
| [5] | Zanos P, Moaddel R, Morris PJ, Riggs LM, Highland JN, Georgiou P, Pereira EFR, Albuquerque EX, Thomas CJ, Zarate CA, Jr. et al: Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms. Pharmacol Rev 2018, 70(3): 621-660. |
| [6] | Schwenk ES, Viscusi ER, Buvanendran A, Hurley RW, Wasan AD, Narouze S, Bhatia A, Davis FN, Hooten WM, Cohen SP: Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med 2018, 43(5): 456-466. |
| [7] | Wang J, Huang J, Yang S, Cui C, Ye L, Wang SY, Yang GP, Pei Q: Pharmacokinetics and Safety of Esketamine in Chinese Patients Undergoing Painless Gastroscopy in Comparison with Ketamine: A Randomized, Open-Label Clinical Study. Drug Des Devel Ther 2019, 13: 4135-4144. |
| [8] | McIntyre RS, Rosenblat JD, Nemeroff CB, Sanacora G, Murrough JW, Berk M, Brietzke E, Dodd S, Gorwood P, Ho R et al: Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. Am J Psychiatry 2021, 178(5): 383-399. |
| [9] | Jonkman K, van Rijnsoever E, Olofsen E, Aarts L, Sarton E, van Velzen M, Niesters M, Dahan A: Esketamine counters opioid-induced respiratory depression. Br J Anaesth 2018, 120(5): 1117-1127. |
| [10] | Zhu M, Xu S, Ju X, Wang S, Yu X: Effects of the Different Doses of Esketamine on Postoperative Quality of Recovery in Patients Undergoing Modified Radical Mastectomy: A Randomized, Double-Blind, Controlled Trial. Drug Des Devel Ther 2022, 16: 4291-4299. |
| [11] | Hung KC, Kao CL, Ho CN, Wu JY, Chang YJ, Lin CM, Chen IW: Efficacy and safety of esketamine in preventing perioperative neurocognitive disorders: a meta-analysis of randomized controlled studies. Syst Rev 2025, 14(1): 68. |
| [12] | Liu J, Wang T, Song J, Cao L: Effect of esketamine on postoperative analgesia and postoperative delirium in elderly patients undergoing gastrointestinal surgery. BMC Anesthesiol 2024, 24(1): 46. |
| [13] | Wu Q, Zhi XJ: Intravenous patient-controlled analgesia versus epidural anesthesia in the treatment of patients undergoing total hip arthroplasty: a retrospective comparative study. BMC Anesthesiol 2025, 25(1): 89. |
| [14] | Myles PS, Myles DB, Galagher W, Boyd D, Chew C, MacDonald N, Dennis A: Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth 2017, 118(3): 424-429. |
| [15] | Ramsay MA, Savege TM, Simpson BR, Goodwin R: Controlled sedation with alphaxalone-alphadolone. Br Med J 1974, 2(5920): 656-659. |
| [16] | Bu XS, Zhang J, Zuo YX: Validation of the Chinese Version of the Quality of Recovery-15 Score and Its Comparison with the Post-Operative Quality Recovery Scale. Patient 2016, 9(3): 251-259. |
| [17] | Woolf CJ, Thompson SWN: The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain 1991, 44(3): 293-299. |
| [18] | Coderre TJ, Melzack R: The contribution of excitatory amino acids to central sensitization and persistent nociception after formalin-induced tissue injury. J Neurosci 1992, 12(9): 3665-3670. |
| [19] | Yao M, Fang B, Yang J, Chen P, Chen F: Esketamine combined with sufentanil versus sufentanil in patient-controlled intravenous analgesia: a meta-analysis. Front Pharmacol 2024, 15: 1247646. |
| [20] | Brinck EC, Tiippana E, Heesen M, Bell RF, Straube S, Moore RA, Kontinen V: Perioperative intravenous ketamine for acute postoperative pain in adults. Cochrane Database Syst Rev 2018, 12(12): Cd012033. |
| [21] | Hudetz JA, Patterson KM, Iqbal Z, Gandhi SD, Byrne AJ, Hudetz AG, Warltier DC, Pagel PS: Ketamine attenuates delirium after cardiac surgery with cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2009, 23(5): 651-657. |
| [22] | Inouye SK, Westendorp RG, Saczynski JS: Delirium in elderly people. Lancet 2014, 383(9920): 911-922. |
| [23] | Min M, Du C, Chen X, Xin W: Effect of subanesthetic dose of esketamine on postoperative rehabilitation in elderly patients undergoing hip arthroplasty. J Orthop Surg Res 2023, 18(1): 268. |
| [24] | Wainwright TW, et al.: Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop 2020, 91(3): 363. |
| [25] | Qu S, Zhang WJ, Zhou HJ, Deng F, Liu RJ, Yan WJ: The efficacy and safety of patient-controlled intravenous analgesia with esketamine after total hip arthroplasty: a randomized controlled trial. BMC Anesthesiol 2025, 25(1): 31. |
| [26] | Crompton J, Osagie-Clouard L, Patel A: Do hip precautions after posterior-approach total hip arthroplasty affect dislocation rates? A systematic review of 7 studies with 6,900 patients. Acta Orthop 2020, 91(6): 687-692. |
| [27] | Hajibandeh S, Hajibandeh S, Bill V, Satyadas T: Meta-analysis of Enhanced Recovery After Surgery (ERAS) Protocols in Emergency Abdominal Surgery. World J Surg 2020, 44(5): 1336-1348. |
| [28] | Li X, He X, Li M, Gu X, Wang P, Wu Y, Chen Y: The effect of esketamine combined with sufentanil based patient-controlled intravenous analgesia for postoperative pain in patients undergoing third molar surgery and maxillofacial trauma: a randomized clinical trial. BMC Oral Health 2024, 24(1): 1460. |
| [29] | Hijazi Y, Boulieu R: Contribution of CYP3A4, CYP2B6, and CYP2C9 isoforms to N-demethylation of ketamine in human liver microsomes. Drug Metab Dispos 2002, 30(7): 853-858. |
APA Style
Shou, Y., Jian-Sheng Luo, Xian-Jie Zhang, Wen-Hu Zhai, Jia Han. (2025). Effect of Esketamine Combined with Sufentanil-Based Patient-Controlled Intravenous Analgesia on Postoperative Pain in Elderly Total Hip Arthroplasty Patients: A Three-Arm Randomized Trial. International Journal of Anesthesia and Clinical Medicine, 13(1), 37-45. https://doi.org/10.11648/j.ijacm.20251301.16
ACS Style
Shou, Y.; Jian-Sheng Luo; Xian-Jie Zhang; Wen-Hu Zhai; Jia Han. Effect of Esketamine Combined with Sufentanil-Based Patient-Controlled Intravenous Analgesia on Postoperative Pain in Elderly Total Hip Arthroplasty Patients: A Three-Arm Randomized Trial. Int. J. Anesth. Clin. Med. 2025, 13(1), 37-45. doi: 10.11648/j.ijacm.20251301.16
AMA Style
Shou Y, Jian-Sheng Luo, Xian-Jie Zhang, Wen-Hu Zhai, Jia Han. Effect of Esketamine Combined with Sufentanil-Based Patient-Controlled Intravenous Analgesia on Postoperative Pain in Elderly Total Hip Arthroplasty Patients: A Three-Arm Randomized Trial. Int J Anesth Clin Med. 2025;13(1):37-45. doi: 10.11648/j.ijacm.20251301.16
@article{10.11648/j.ijacm.20251301.16,
author = {Yu-Hang Shou and Jian-Sheng Luo and Xian-Jie Zhang and Wen-Hu Zhai and Jia Han},
title = {Effect of Esketamine Combined with Sufentanil-Based Patient-Controlled Intravenous Analgesia on Postoperative Pain in Elderly Total Hip Arthroplasty Patients: A Three-Arm Randomized Trial
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {1},
pages = {37-45},
doi = {10.11648/j.ijacm.20251301.16},
url = {https://doi.org/10.11648/j.ijacm.20251301.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251301.16},
abstract = {Background: Total hip arthroplasty (THA) is a common procedure for end-stage hip disorders, yet postoperative pain management remains challenging due to opioid-related complications, particularly in elderly patients vulnerable to respiratory depression and delirium. Multimodal analgesia strategies are increasingly prioritized to mitigate these risks. Esketamine, an NMDA receptor antagonist with opioid-sparing and anti-neuroinflammatory properties, shows promise in enhancing analgesia while reducing adverse effects. Preliminary studies suggest its efficacy in lowering postoperative pain and delirium risk, though optimal dosing in elderly THA populations remains unclear. This study aimed to evaluate the analgesic efficacy and safety of different dosages of esketamine combined with sufen-tanil for patient-controlled intravenous analgesia (PCIA) in elderly patients undergoing total hip arthroplasty. Methods: In this randomized, prospective, double-blind trial, 120 elderly patients were randomly divided into three groups: the control group (Group S, n = 40) received sufentanil 2 μg/kg; the experimental group SE1 (n = 40) received sufentanil 1.5 μg/kg combined with esketamine 1 mg/kg; and the experimental group SE2 (n = 40) received sufentanil 1 μg/kg combined with esketamine 2 mg/kg. Primary outcomes included resting and movement-associated Visual Analogue Scale (VAS) scores at 4, 8, 12, 24, and 48 h postoperatively. Secondary outcomes encompassed Ramsay Sedation Scale (RSS) scores, Quality of Recovery-15 (QoR-15) scores at 48 h, time to first walk, the number of patients requiring remedial analgesia, and adverse events (nausea/vomiting, hallucinations, pruritus, delirium, dizziness). Results: The SE1 and SE2 groups demonstrated significantly superior analgesic efficacy compared to the S group across all outcomes. Resting and movement-associated VAS scores were significantly lower in both esketamine-combined groups at all postoperative time points (4, 8, 12, 24, and 48 h; P P P P P P P < 0.05) in Groups SE1 and SE2 compared to Group S, with no significant differences in dizziness, hallucinations, or pruritus. Conclusion: This randomized controlled trial demonstrated that esketamine combined with reduced-dose sufentanil significantly improved postoperative analgesia and recovery outcomes in elderly patients undergoing THA.
},
year = {2025}
}
TY - JOUR T1 - Effect of Esketamine Combined with Sufentanil-Based Patient-Controlled Intravenous Analgesia on Postoperative Pain in Elderly Total Hip Arthroplasty Patients: A Three-Arm Randomized Trial AU - Yu-Hang Shou AU - Jian-Sheng Luo AU - Xian-Jie Zhang AU - Wen-Hu Zhai AU - Jia Han Y1 - 2025/05/09 PY - 2025 N1 - https://doi.org/10.11648/j.ijacm.20251301.16 DO - 10.11648/j.ijacm.20251301.16 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 37 EP - 45 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20251301.16 AB - Background: Total hip arthroplasty (THA) is a common procedure for end-stage hip disorders, yet postoperative pain management remains challenging due to opioid-related complications, particularly in elderly patients vulnerable to respiratory depression and delirium. Multimodal analgesia strategies are increasingly prioritized to mitigate these risks. Esketamine, an NMDA receptor antagonist with opioid-sparing and anti-neuroinflammatory properties, shows promise in enhancing analgesia while reducing adverse effects. Preliminary studies suggest its efficacy in lowering postoperative pain and delirium risk, though optimal dosing in elderly THA populations remains unclear. This study aimed to evaluate the analgesic efficacy and safety of different dosages of esketamine combined with sufen-tanil for patient-controlled intravenous analgesia (PCIA) in elderly patients undergoing total hip arthroplasty. Methods: In this randomized, prospective, double-blind trial, 120 elderly patients were randomly divided into three groups: the control group (Group S, n = 40) received sufentanil 2 μg/kg; the experimental group SE1 (n = 40) received sufentanil 1.5 μg/kg combined with esketamine 1 mg/kg; and the experimental group SE2 (n = 40) received sufentanil 1 μg/kg combined with esketamine 2 mg/kg. Primary outcomes included resting and movement-associated Visual Analogue Scale (VAS) scores at 4, 8, 12, 24, and 48 h postoperatively. Secondary outcomes encompassed Ramsay Sedation Scale (RSS) scores, Quality of Recovery-15 (QoR-15) scores at 48 h, time to first walk, the number of patients requiring remedial analgesia, and adverse events (nausea/vomiting, hallucinations, pruritus, delirium, dizziness). Results: The SE1 and SE2 groups demonstrated significantly superior analgesic efficacy compared to the S group across all outcomes. Resting and movement-associated VAS scores were significantly lower in both esketamine-combined groups at all postoperative time points (4, 8, 12, 24, and 48 h; P P P P P P P < 0.05) in Groups SE1 and SE2 compared to Group S, with no significant differences in dizziness, hallucinations, or pruritus. Conclusion: This randomized controlled trial demonstrated that esketamine combined with reduced-dose sufentanil significantly improved postoperative analgesia and recovery outcomes in elderly patients undergoing THA. VL - 13 IS - 1 ER -
Department of Anesthesiology, Deyang People’s Hospital, Deyang, China;School of Medical and Life Sciences, Chengdu University of Traditional Chinese Medicine, Chengdu, China
Department of Anesthesiology, Deyang People’s Hospital, Deyang, China
Department of Anesthesiology, Deyang People’s Hospital, Deyang, China
Department of Anesthesiology, Deyang People’s Hospital, Deyang, China
Department of Anesthesiology, Deyang People’s Hospital, Deyang, China;School of Medical and Life Sciences, Chengdu University of Traditional Chinese Medicine, Chengdu, China